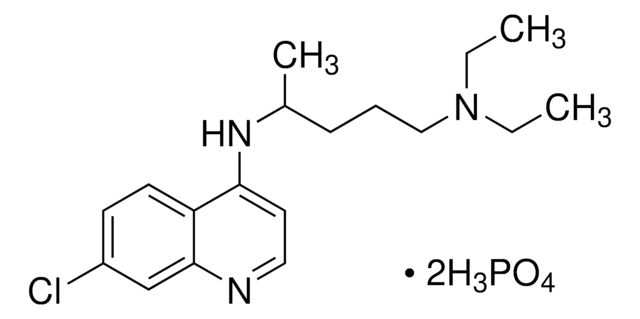
Chloroquine effectively eliminates the erythrocytic forms of malaria parasites at all developmental stages, although it does not impact the sporozoites. It also functions as an antibiotic. In addition, it can be utilized at a concentration of 200 mg/mL (PBS, pH 5.0) to dissociate antigen-antibody complexes without denaturing red blood cell antigens. Recent research indicates chloroquine′s potential as an antitumor medication for cancer treatment along with chemotherapy and radiation. Its antimalarial effects are achieved by inhibiting the polymerization of heme into hemozoin, which serves as a food source for the malarial parasite. Chloroquine forms a complex with the drug-hemozoin, capping the polymerizing chain and preventing further polymerization. As a result, free heme accumulates in the food vacuole, exerting toxic effects on the parasite. Additionally, chloroquine acts as an anti-autoimmune therapy by binding to transcriptional factors on T helper 17 cells and inhibiting their differentiation.
[1] Chloroquine diphosphate (CQ) is frequently employed as an inhibitor of the autophagic pathway. The combined use of chloroquine diphosphate and salidroside initiates apoptosis in human liver cells by modulating mitochondrial dysfunction and autophagy.
[2]Chloroquine is a member of quinolone family
[3] and is a weak intercalating agent.
[4] Chloroquine is used for treating amebiasis, rheumatoid arthritis, discoid and systemic lupus erythematosus.
[5]